Skip to main content
Skip to footer
Reviews
Request an Appointment
Colonoscopy Patient Instructions
Patient Portal
Contact Us
About Us
Providers
Locations
Services
Axonics Therapy
Bravo pH Monitoring System
Capsule Endoscopy
Colonoscopy
EGD – Upper GI Endoscopy
ERCP
Esophageal Manometry
Hemorrhoid Banding
HemWell
Ideal Protein
Infusion Therapy
PEG/PEJ
Sigmoidoscopy
Research
Forms
Colonoscopy Patient Instructions
Patient Forms
Patient Resources
Procedure Prep
Referring Physician
What to Expect
Insurance
Resources
About Us
Providers
Locations
Services
Axonics Therapy
Bravo pH Monitoring System
Capsule Endoscopy
Colonoscopy
EGD – Upper GI Endoscopy
ERCP
Esophageal Manometry
Hemorrhoid Banding
HemWell
Ideal Protein
Infusion Therapy
PEG/PEJ
Sigmoidoscopy
Research
Forms
Colonoscopy Patient Instructions
Patient Forms
Patient Resources
Procedure Prep
Referring Physician
What to Expect
Insurance
Resources
Find a Provider
Find a Location
Blogs
Blog Categories
All
Articles
Diet Resources
Pediatrics Resources
Pediatrics Resources
“Mama, I Don’t Feel Good…”: Children’s Digestive Issues
Pediatrics Resources
Growing the Wrong Way
Articles
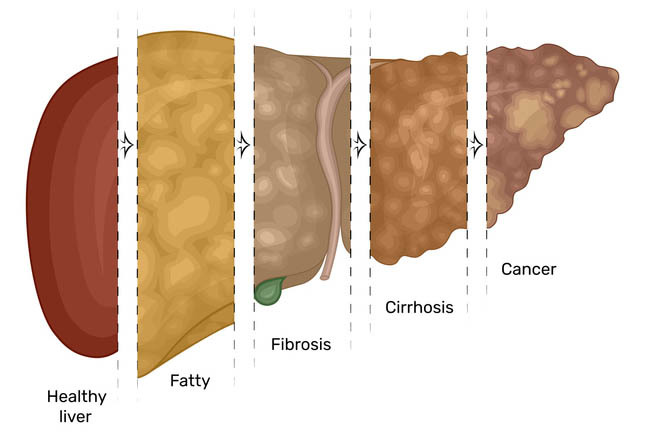
Four Major Concerns of the Liver
Articles
Simple Strategies for Protecting Your Liver Health
Articles
The Importance of the Liver in Our Body
Articles
Hope on the Horizon: Breakthroughs in Hepatitis Treatment
Articles
Avoid the Transmission: Understanding the Different Types of Hepatitis
Articles
Spread the News, Not the Disease: Hepatitis Awareness Month
Diet Resources
Food That Will Keep the Gut Happy
Articles
Celebrating the Advancements of Pancreatic Cancer Research
Articles
The Importance of Pancreas Mainten-eas
Articles
Pancreas 101: Understanding and Caring for Your Pancreatic Health
Articles
Keeping Colon Disease at Bay During This Christmas Season
Articles
Preparing for a Flexible Sigmoidoscopy?
Articles
Protecting Your Colon This Holiday Season
Articles
The Effect of Holiday Stress on the Gastrointestinal System
Articles
Concerns about Barrett’s Esophagus
Articles
Trick or Treat: The Effect of Candy on Your Gastrointestinal System
Articles
Understanding the Dangers of Obesity
Diet Resources
Concerns of Growth in Childhood Obesity
Articles
Can Probiotics Assist with Gastroparesis Prevention?
1
2
Request An Appointment
Find a Provider
Find a Location
About Us
Providers
Locations
Services
Axonics Therapy
Bravo pH Monitoring System
Capsule Endoscopy
Colonoscopy
EGD – Upper GI Endoscopy
ERCP
Esophageal Manometry
Hemorrhoid Banding
HemWell
Ideal Protein
Infusion Therapy
PEG/PEJ
Sigmoidoscopy
Research
Forms
Colonoscopy Patient Instructions
Patient Forms
Patient Resources
Procedure Prep
Referring Physician
What to Expect
Insurance
Resources
Request an Appointment
Pay My Bill
Patient Portal
Contact Us
Colonoscopy Patient Instructions